
OLD MODEL -vs- NEW MODEL:
THE COLLAGEN / SCAR TISSUE REMODELING ‘SUPER PAGE‘
Collagen is a protein. Other than water, it is the most abundant material found in Connective Tissue. Approximately 1/3 of all protein in the body is collagen. What makes this protein so useful is its dual advantages of being able to supply both strength and elasticity, while resisting over-stretching (injury).
Unlike most proteins, which form clumps when gathered together, collagen is fibrous and can form mats (like APONEUROSIS), sheets (like FASCIAL MEMBRANES), or chord-like structures (TENDONS and MUSCLES). It also has the ability to act as an adhesive. The word itself comes from the Greek language and means “Glue Producer”.
Although there are almost 30 different kinds of collagen, it is Type I Collagen that interests us because it is the kind found in what I refer to as the Elastic, Collagen-Based Connective Tissues (Ligaments, Tendons, Muscles, and Fascia — yes, I realize that muscles are not technically connective tissues). Thus, collagen is the substance that “glues” or “connects” the various parts of the body together. This is why so many of the collagen-based tissues in the body are generically known as “Connective Tissues”.
Some collagen-based connective tissues like bone and most cartilages, are part of your body’s load-bearing framework. Their purpose is to withstand compressive forces, while grossly maintaining the body’s shape. On the other hand, you have the Elastic, Collagen-Based, Connective Tissues, whose chief job is overcome the tensile forces that are constantly trying to pull the body apart. These must be able to stretch; and include tissues like ligaments, tendons, muscles, and fascia, or be able to withstand compressive loads, such as articular cartilage (which is not the focus of this page). Collagen fibrils have a spring-like quality both in their structure and function.
When healthy, these elastic, collagen-based tissues are all similar (ligaments and tendons, tend to be less elastic than fascia and muscles). However, if you were to look at any of these tissues under a microscope, you would notice that the individual collagen fibers all align themselves in a very orderly and organized parallel fashion to each other — sort of like well-combed hair. When we put lots of these collagen fibrils together, we get tissue with a “wave-like” appearance. The wavy quality of collagen is what gives it both strength, and the incredible ability to elast and stretch.
COLLAGEN FIBRILS ARE WOVEN INTO SHEETS, BANDS, OR CORDS, AND FOLLOW THE “TUBE-WITHIN-TUBES” MODEL
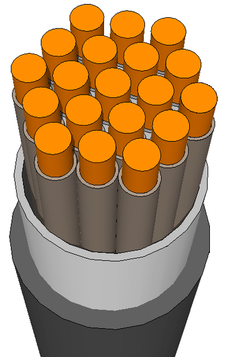
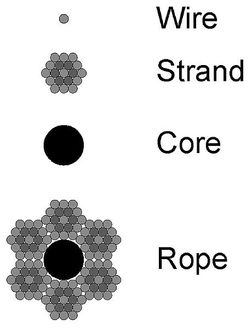
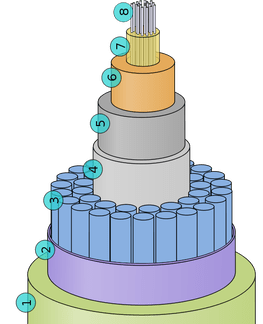
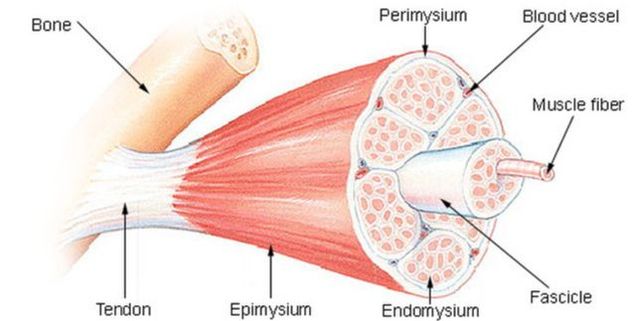
Connective tissues follow a tubes-within-tubes model. For example, both tendons and muscles have bundles within them called fascicles. Within these bundles of fascicles are fibrils. Within fibrils are subfibrils, and then come structures called microfibrils. These tiny fibers are made up of collagen molecules that are composed of chains and cross-links. This is just one of the reasons that collagen is so strong. Fascia is arguably the most amazing of these collagen-based connective tissues.
Virtually every tissue in your body is wrapped in some form of Fascia. The entire body is covered with Fascia from head to toe. Individual muscles are then wrapped in fascia. Groups of muscles, nerves, blood vessels, organs, as well as other tissues are further wrapped up in fascia. In other words, all of the individual tubes have their own layer of Fascia that they are wrapped inside.
Just understand that collagen’s ability to cross-link is a double edged sword. Like a net, the more cross-links there are, the stronger the tissue is. But in the body, there is always a give and take. As we have all experienced; the stronger the rope, the less flexible it will be. When these elastic, collagen-based connective tissues are injured by OVERUSE (jobs, sports, etc) or trauma (sports, CAR WRECKS, etc), or even CRAPPY POSTURE, they can become disorganized and tend to take on a “WOVEN BASKET” appearance microscopically.
We end up with tissues whose microscopic fibers run every which way, in all three dimensions. The injured tissue becomes very disorganized, with individual fibers acting more like a wadded up and tangled “HAIRBALL” than well-combed hair. As you can imagine, this “micro-scarring” (the medical community calls it “FIBROSIS“) is a big problem.
NORMAL TISSUE -VS- SCAR TISSUE
 |  |  |
Look at the difference in the microscopic appearance of the pictures above. The pics on the left and right represent the unorganized and dysfunctional aspect of microscopic scarring and fibrosis. However, if you look closely at the pic in the middle, you can see the wave-like structure of the tissue as well as the wavy collagen fibrils that I overlapped into the pic.
Do you think that the unorganized nature of scar tissue could cause it to be restrictive as far as its ability to move, stretch, and elast? You better believe it! Surround a joint with this stuff and you end up with problems — big problems!
You see, abnormal joint motion is the known cause of JOINT DEGENERATION (thinning discs or joint spaces, bone spurs, and calcium deposits). Any relief of symptoms without actually breaking adhesion and restoring motion is temporary at best. Yet this is what our medical community is largely based on.
Run lots of tests, tell you that nothing is really wrong with you other than maybe old age and some ‘arthritis’, prescribe drugs, repeat. No wonder this short-sighted approach never works! If you have been on this MEDICAL MERRY-GO-ROUND, you already know this. I always wonder when the mainstream will figure out there’s a huge difference between FUNCTIONAL DEFICITS & PATHOLOGY that cannot be ignored or brushed aside with insulting explanations?
HEALING AND REPAIR OF COLLAGEN-BASED TISSUES
Dr. James Cyriax (1905-1985) was a British doctor who is considered to be the, “Father of Orthopedic Medicine”. In 1929, Dr. Cyriax grew frustrated with the fact that there were not good methods of diagnosing and treating problems of the soft tissues. In response to this dilemma, he developed a system to both diagnose injuries of the musculoskeletal system and treat them non-surgically. It was Cyriax who brilliantly stated, “All pain has a source, and all treatment must reach the source.”
Although Cyriax’ theories were certainly not new, and various forms of soft tissue treatment had been around for thousands of years, his work was the spark that lit a fire under the medical community to begin researching connective tissue injuries and the best methods of treating them. Over the past forty years, there has been an incredible surge in the study of connective tissues, injury mechanisms, diagnosis, long term effects, as well as the proper treatment of these injuries. Unfortunately, too many clinicians are practicing according to the old and outdated models.
Current scientific literature is chocked full of the beneficial effects of “Controlled Loading” on the Elastic, Collagen-Based Connective Tissues. This “Controlled Loading” that I often refer to as “Controlled Trauma” (breaking down the microscopic scarring so frequently found in these soft tissues causes FIBROBLASTIC PROLIFERATION). In doctor lingo, “blasts” are “builders”). Fibroblasts are responsible for manufacturing and taking care of collagen, fibronectin, proteoglycans and other proteins that make up Connective Tissues.
Additionally, we know that “Controlled Loading” causes a resorption of restrictive and fibrotic tissue that is found in Microscopic Scar Tissue and Adhesions. In other words, the Scar Tissue Remodeling Treatment that we do for injured, Collagen-Based Connective Tissues not only helps to break down the scarred area so that it can be reabsorbed by the body; it causes the cells that create new collagen to increase in both number and activity.
VASCULAR DISRUPTION & BRUISING
As crazy as it might seem, it is critical to create a vascular disruption of the microscopic scar tissue. In order to start the body’s natural healing processes, we have to start an Inflammatory Cascade, and in order to start the Inflammatory Cascade we have to disrupt the scar tissue’s blood supply. Although too much inflammation is certainly a bad thing (SYSTEMIC INFLAMMATION —- an out-of-control health issue that is responsible for much if not most of America’s ill health), a precisely localized inflammation is actually part of the body’s normal immune system response. It is not only good, it is necessary for healing to take place.
This inflammatory response that comes from the “BREAKING” and BRUISING that is characteristic of our Scar Tissue Remodeling, and what ultimately leads to the “Remodeling Phase” of tissue repair, as well as new collagen formation along the body’s normal LINES OF MECHANICAL STRESS / LOAD. Even though scar tissue is not something you ultimately want to have in your body; it is frequently the best your body can provide under the circumstances.
Just remember that this scar tissue is living tissue with a blood supply. When the adhesed tissue is broken (“Controlled Loading“), the capillary beds that supply blood to the tissue also break. This causes an internal leakage of red blood cells into the surrounding tissue. In plain old English, you’ll have a bruise. This is why we tell our patients to “EMBRACE THE BRUISE“.
Following the Controlled Loading with Tensile Loading (STRETCHING) has been proven to cause an increase in proteoglycan and collagen synthesis within the injured area(s) as well. This is why when your treatment is complete, and you have finished your “Initial Intensive” Stretching Protocol; it is important to engage in some resistance training for the affected area, as well as a “MAINTENANCE” Stretching Protocol.
You may have heard (especially if you were injured in a Motor Vehicle Accident, and are being hounded by an insurance company) that injuries to the Elastic, Collagen-Based “Soft Tissues” take, at the most, 6-8 weeks to heal. This is true — only if you strictly limit your definition of the word “heal”.
When injury to the Elastic, Collagen-Based Connective Tissues (ligaments, tendons, muscle, fascia, etc) takes place, there are four distinct phases of healing that the body must go through. And although the first three are largely accomplished in the first month, it is the fourth and most critical stage that we are chiefly interested in as it is most related to chronic pain and dysfunction.
THE PHASES / STAGES OF TISSUE REPAIR & HEALING
STAGE I (Inflammatory Phase):
This phase lasts from 12-72 hours, and is characterized by a release of inflammatory chemicals by injured cells. When cells are injured and die, they rupture and release their contents into the extracellular fluid. This causes the body’s Immune System to release the chemicals we know as “Inflammation” (HERE).
Excessive amounts of Inflammation can cause a great deal of pain. They also promote excessive microscopic scarring (HERE). Be aware that if you visit your doctor for a soft tissue injury, you will be given anti-inflammatory medications (NSAIDS). Although it would logically seem the thing to do, these drugs have serious side-effects (heart, liver, kidneys, etc). However, the real kick in the teeth is the fact that this they have been scientifically proven to cause injured connective tissues to heal significantly weaker and with less elasticity than they otherwise would. Nowhere is this more true than with CORTICOSTEROIDS.
Do a quick search of the Medico-Scientific Literature on Corticosteroids and soft tissue injuries, and you will see over and over and over again that they are detrimental to the healing process of soft tissues and should play no part in the treatment of these injuries.
STAGE II (Passive Congestion):
In this phase that begins by the 2nd or 3rd day, we begin to see swelling (sometimes we do not see it, because it is not on the body’s surface). Remember; “inflammation” is not synonymous with swelling. Inflammatory Chemicals released by your body due to dying cells attract the fluid that causes swelling. This is why using cold therapy (ICE) to control both inflammation and swelling is such an important part of the healing process — particularly in its earliest stages.
STAGE III (Repair Phase):
The Repair Phase is where new collagen fibers are made by fibroblasts. Like we talked about earlier, this collagen has the ability to take on two distinctly different forms; fiber or glue. Fiber and glue, fiberboard and plaster, pressboard and adhesive, chicken wire and stucco, re-bar and concrete…. These are a few common examples of this concept from the construction industry. The human body is actually quite similar. The body then uses these collagen fibers as a sort of soft tissue “patch” — a patch that provides a degree of strength and elasticity. Just like your old blue jeans, a patch is not ideal. But once those old Levis tear or rip, what else are you going to do?
Unfortunately, in the body, this collagen patch (SCAR TISSUE) tends to be different than the tissue around it in a number of ways. Scar Tissue is weaker, less elastic, much more pain sensitive (HERE), and has SEVERELY DIMINISHED PROPRIOCEPTIVE ABILITIES. Be aware that the Repair Phase of tissue healing only lasts 6 weeks, with the vast majority being completed in the first three.
WARNING: This 3rd stage of healing is where many of the so-called “experts” (i.e., the insurance company of the guy who hit you) want you to believe the whole process of Tissue Healing & Repair ends.
STAGE IV (Remodeling Phase):
Although it is typically the least talked about, the Remodeling Phase is by far the most critical of the four stages of Connective Tissue healing. It is also where people most often get duped (sometimes inadvertently, but more often than not, purposefully) by doctors, insurance companies, and attorneys. Many of you reading this know exactly what I am talking about.
Research clearly shows that in cases of serious Connective Tissue Injury, the Remodeling Phase can last up to (gulp) two years or more; making the old “6-8 weeks” sound ridiculous. The Remodeling Phase is characterized by a “realignment” (remodeling) of the individual fibers that make up the injured tissue (the collagen “patch” I so often refer to as SCAR TISSUE).
As Controlled Loading / Tensile Loading is applied to the healing tissues via chiropractic adjustments, Tissue Remodeling, STRETCHING and strengthening exercises, PROPRIOCEPTIVE RE-EDUCATION, massage therapy, TRIGGER POINT THERAPY, PNF, etc; the individual tissue fibers move from a more random, tangled, and twisted wad of unorganized and “TETHERED” collagen fibrils; to a tissue that is much more organized, parallel, and orderly as far as its microscopic configuration is concerned. Again, this takes time!
Although our Scar Tissue Remodeling Therapy can frequently bring immediate relief (just look at our VIDEO TESTIMONIALS), it is obvious from the medical literature that there are healing processes taking place that simply cannot be bypassed.
CONNECTIVE TISSUE HEALING (The Final Word):
Everyone has heard the old cliche that is still used by doctors, “You’d have been better off to break the bone than to tear the ligaments“. Knowing what we know about the healing of the Collagen-Based, Elastic Connective Tissues; this statement makes a lot of sense! Soft tissues heal much slower than other tissues (including bones). Do not let anyone try and convince you otherwise! This is why following the complete stretching and strengthening protocol that goes hand-in-hand with our “Tissue Remodeling” treatment, is the one and only way that it will work properly over the long haul.
As you will notice from our YOUTUBE PAGE, many people have almost immediate relief of CHRONIC PAIN after a single treatment. I am always thrilled by this! However, be aware that complete healing of the injured tissue (including remodeling) is going to take several months at the very least. What does this mean for you, the patient?
It means that there is always an increased risk of re-injury in an area that has been injured previously. No matter how good you feel after treatment, stay on track and follow your treatment protocol (THIS IS NOT WHAT I MEAN). Oh, and for those of you whose situation is much more complex, READ THIS.
SCAR TISSUE IS DIFFERENT THAN NORMAL TISSUE BECAUSE………
Microscopic scar tissue is problematic because it is so dramatically different than healthy connective tissue in a number of different ways:
SCAR TISSUE IS WEAKER:
As you can imagine, the tangled “clump” of tissue that characterizes a microscopic scar, is far weaker than normal connective tissue. You already know this. Sprain an ankle, and it is easier to sprain it again and again and again. This information is common knowledge and can be found in any Pathology Textbook.
SCAR TISSUE IS LESS ELASTIC:
This is another no-brainer. A HAIR BALL is less elastic than well-combed hair. Look at it another way. Put your hands out in front of you on a table top, with the fingers facing each other. Now run the fingers from one hand, back and forth, between the fingers from the other hand. Notice how the fingers glide? Now run your fingers from one hand to the other, and ball up your fingers. This is what tangled and twisted connective tissues do microscopically. They are extremely restrictive and subsequently, they loose their stretchiness and elasticity. This is also common knowledge, and can be found in any Pathology Textbook.
SCAR TISSUE DOES NOT OXYGENATE WELL, CREATING A LOW (acidic) PH:
Known as hypoxia, decreased oxygenation is terribly harmful because oxygen is critical for proper tissue healing to occur. When connective tissues are injured, swelling occurs; and it is this combination of swelling and twisted / tangled tissue that restricts the blood flow and oxygen supply to the connective tissues. Lack of OXYGEN also creates a very acidic environment, which is detrimental not only to the healing process of the Elastic, Collagen Based Connective Tissues (ligaments, tendons, muscles and fascia), but to health in general. This fact is well known by doctors and can likewise be found in all Pathology Textbooks.
SCAR TISSUE IS DIFFERENT NEUROLOGICALLY:
It is easy to see how microscopic scarring is different mechanically and chemically. What most doctors fail to tell you (many do not realize or understand this concept) is that scar tissue is different neurologically as well. Why don’t doctors ever talk about this aspect of tissue injury? The information has not been around long enough to get into the textbooks. The latest scientific research tells us that the nerves in scar tissue can conduct pain up to 1,000 times more effectively than the same nerves in normal tissue.
Stop!
If you are truly interested in understanding chronic pain, re-read the last few sentences a couple times and let it sink in. This hyper-conductivity of the nerve system creates what is known as TYPE III PAIN (SUPER-SENSITIVITY), which in many cases today is known by another name; CENTRAL SENSITIZATION.
Abnormally functioning nerves in scar tissue, leads to all sorts of degenerative problems such as DJD. It can also lead to “Hyperalgia” (extreme sensitivity to pain —– stimulus that should cause a little pain causes extraordinary amounts of pain), or “Allodynia” (stimulus which would not normally cause any pain, now causes pain). In people dealing with copious amounts of underlying scar tissue, these two frequently overlap.
WARNING WARNING WARNING
SYSTEMIC CONNECTIVE TISSUE PROBLEMS ARE A DIFFERENT KIND OF ANIMAL
Not all cases of Connective Tissue Problems (Fascial Tears & Adhesions, Tendinosis, Ligament Injuries, or Muscle Problems) are rooted in purely mechanical causes. There are all sorts of things that can create an environment within the body that can lead to a systemic problem with certain Connective Tissues.
As you might imagine, bilateral Tendinosis, Tendinosis at multiple sites, Fascial Adhesions over wide areas of the body, muscle problems all over the place, all begin to raise some red flags concerning this issue (HERE, HERE, and HERE). Not that it is always the case, but when I see these situations during examination, I began to question whether there might be a deeper problem — a “Systemic” or whole body problem.
Very frequently, the underlying systemic problem turns out to be some sort of AUTOIMMUNE DISEASE. If for whatever reason, your body is making antibodies to attack it’s own tendons (since most tendinopathies are not considered “inflammatory,” increasing numbers of experts are postulating this as a cause), muscles, fascia, or ligaments, you have a serious problem on your hands — a problem that will not respond to the Scar Tissue Remodeling Treatments that I do. Or at least not for very long.
And I promise that this nightmare will not stop with your Connective Tissues. If you want to get a handle on Autoimmunity and its relationship to potential problems of the Elastic, Collagen-Based Connective Tissues, please read some of the posts filed under the previous link.
CONNECTIVE TISSUE INJURY, COLLAGEN HEALING, REPAIR, & REGENERATION….
NEW MODEL -vs- OLD MODEL
Depending on whose research you believe, anywhere from 50 to 100 million Americans suffer with Chronic Pain. This means that at a bare minimum, one in four American adults is dealing with some type of Chronic Pain issue that despite who-knows-how-many doctor visits, untold numbers of diagnostic tests, and an obscene outlay of cash (both private and public); has proven impossible to solve.
Although Chronic Pain comes in a wide variety of shapes, sizes, and flavors, the most common type of Chronic Pain — the type of pain known as Deep Somatic Pain — originates in the Elastic, Collagen-Based Connective Tissues (as well as bone or vascular tissue). Some of these elastic tissues have names you are very familiar with (muscles, tendons, ligaments). Some have names you may have never heard of before (fascia). Allow me to stop for a moment and speak about briefly fascia.
Although everyone has heard of tissues like tendons, muscles, and ligaments; only those in health care have likely heard of fascia. Fascia is the thin, white-yellow, almost translucent membrane, that covers muscles. You have seen it on a pot roast (or the last deer you skinned — around here, hunters call it “striffin”). Fascia not only “wraps” or covers the whole body, it also covers each individual muscle, bundles of muscle fibers inside a muscle, groups of muscles, nerves, blood vessels, and organs. Metaphorically speaking, fascia is the “cellophane” that holds the sandwich together!
Because most fascial membranes are as thin as paper, they do not image well on diagnostic tests —– even the most technologically advanced imaging such as MRI (HERE). Those of you who deal with chronic Deep Somatic Pain know all too well what this means. Because fascia does not image with even the most advanced techniques such as MRI (HERE), it is not on the radar virtually any of the medical community. Out of sight – out of mind!
This might not be such a big deal if it were not for a couple of very important facts. Fascia is not only the single most abundant Connective Tissues in the body, but it also happens to be one of the most pain-sensitive tissues as well. In fact, I have seen different sources state that fascia is arguably the single most pain sensitive tissue in the human body.
What happens when you add these facts together? A recipe for disaster. A recipe for Chronic Pain! The most pain sensitive tissue in the body (fascia) + abundant amounts of it everywhere (and I do mean everywhere) + an inability to image with even the most advanced diagnostic imaging technologies = deer-in-the-headlight looks from your doctor.
I know that many of you reading this can relate to being treated like you are a hypochondriac or drug seeker, and being told that there is nothing really wrong with you other than the fact that, “You have a little arthritis. I mean, after all Mrs Jones; you just aren’t as young as you used to be” — something I discussed at length HERE.
Don’t get me wrong, not all Chronic Pain is of the Deep Somatic type; some of it is related to misfiring of nerves in the central or peripheral nervous system — another topic for another day. However, twenty five years of clinical experience has shown me that huge numbers of people suffer with this type of pain can usually be helped — if it is treated using the correct model. And if I am not sure? TRY A TREATMENT AND SEE!
Unfortunately, far too great a percentage of the medical community is living in the past, and not treating collagen-based tissues properly. Many are still using The Old Model; a model based on resting injured tissues and PRESCRIBING “THE BIG-FIVE”.
THE RELATIONSHIP BETWEEN COLLAGEN-BASED TISSUES, INFLAMMATION, AND PAIN
As we learned in Part II, fascia is one of the most abundant of the Elastic, Collagen-Based Connective Tissues in the human body. It is also, arguably, the most potentially pain-sensitive. On top of all this, it does not show up on even the most technologically advanced diagnostic imaging — i.e. MRI, CT, etc. Those of you who suffer with Chronic Pain have figured out that this does not bode well for your doctor visits.
You end up with lots of diagnostic imaging and other tests that tell the doctor absolutely nothing about what is causing your pain. The end result is that they want you to do even more diagnostic testing. And, of course, there is always the recommendation for more drugs. This is because the medical community is still treating injuries to the Elastic, Collagen-Based Connective Tissues using a model that was outdated a generation ago
THE OLD MODEL OF COLLAGEN REPAIR
The old model of connective tissue injury (prior to the 1980′s) was partially correct. Overuse (repetitive injury) or traumatic injury caused cell death. When cells die, they rupture their contents (chemicals) into the extracellular fluid — the fluid that bathes the outside of all cells. Many of these chemicals that were not a problem on the inside of the cell, suddenly become noxious irritants when they are outside of the cell. On top of this, numerous Immune System chemicals are released by the body to perform the complex process of removing these chemicals in order to get the healing process rolling. This process is called Acute Inflammation.
Although these inflammatory chemicals are a necessary (even vital) part of the normal healing process, too many of these chemicals in one place cause things like excess pain and dysfunction —– and excess microscopic scarring. Be warned that although we are talking about Acute Inflammation here, there is something called Chronic Inflammation that can be an even bigger problem. I will touch more on Inflammation in the final chapter.
According to the old model of tissue injury, the real culprit in most people’s pain and dysfunction is those pesky inflammatory chemicals. These inflammatory chemicals have big names like cytokines, leukotrienes, prostaglandins, histamines, and numerous others. Let me reiterate: It’s not that these “chemicals of inflammation” are bad. The truth is, they are a critical component of any normal healing process. It’s just that when they are present in abnormally large amounts (or for abnormally long periods of time), they begin to create problems — lots of problems.
The Cardinal Signs of localized inflammation are always given in Latin and include:
- RUBOR (Redness)
- DOLAR (Pain)
- CALOR (Heat)
- TUMOR (Swelling)
- FUNCTIO LAESA (Loss of Function)
Everyone has experienced this process. Sprain an ankle, tweak your back, or get rear-ended while sitting at a stop light, and what happens? The tissues (cells) that were injured severely enough, die, and then rupture their contents into the extracellular fluid. The cells contain inflammatory chemical mediators, which, once released, attract fluid to the area (TUMOR).
Because of excess blood flow and fluid effusion into the tissue, there is often RUBOR & CALOR as well. All of this causes DOLAR, and leads to the formation of microscopic scar tissue and FUNCTIO LAESA. Hopefully it all clears up quickly……. Hopefully. I say hopefully, because how are injuries to the Elastic, Collagen-Based Connective Tissues treated under our current medical system? According to the Old Model of course!
People head to the doctor, and the tech takes a bunch of X-rays. Or maybe they decide that an MRI OR CT SCAN is in order. We already have a problem. If you remember what we learned in Part II; diagnostic imaging does an exceedingly poor job of imaging these soft tissues — particularly the most pain sensitive of the bunch — fascia. The doctor comes into the room and says, “Thank God Mrs. Jones — nothing is broken. You are free to go. Take these medications.” This is the Old Model. Do you see any problems with this model?
When it comes to dealing with injuries to the Elastic, Collagen-Based Connective Tissues (ligaments, tendons, muscles, and fascia), you’ve seen that the medical community is frequently living in the past. One way we can actually tell this by the way that Connective Tissue Injuries are named. The word “itis” means inflammation. Think about how many musculoskeletal problems with the ability to cause Chronic Pain are named in such a manner as to imply that their primary cause is inflammation. Tendon(itis), Burs(itis), Arthr(itis), Tenosynov(itis), fasci(itis), etc, etc, etc.
This fact alone reveals that most of the medical community is treating according to a model that was outdated at least 20 years ago. They are burying their heads in the sand concerning the scientific research that is pouring forth from their own profession, and going about the business of treating these soft tissue problems via prescription. According to the Old Model, the real problem is Acute Inflammation. If we can just control inflammatory chemicals (see Part III), we can control pain.
The problem is that neither pain nor inflammatory chemicals are the root of the problem — they are merely symptoms. What is the real problem here? It is easy to see. The underlying cause of so many patient’s symptoms is the tissue injury. Take care of the injury and you begin to address the underlying cause of the symptoms. But how are injuries most often treated using the Old Model? Anti-inflammation drugs of course!
Anti-inflammatory drugs have been around for a very long time. And never let it be said that they do not work. Many of them work like magic. However, just like you saw in Lord of the Rings, there is a steep price to be paid for using that magic. Are you willing to pay for pain relief with your heart? How about your liver? What about your digestive tract? How about some dialysis (complete kidney failure)? How about some osteoporosis, or degenerative arthritis, or God only knows what else? These are just a few of the costs of using anti-inflammatory drugs! A half hour of online research will show you that this problem is as serious as a heart attack — literally!
It was the infamous Vioxx debacle of 2004 that started the American drug-consuming public wondering about anti-inflammation medications. No one really knows how many people died as a direct result of Vioxx, but extrapolated data suggests that 150,000 people suffered heart attacks and as many as 60,000 may have died.
Although I could write a book on the topic of DANGEROUS DRUGS, I am not here to talk about the multitudes of organic (organ) problems associated with anti-inflammation drugs. I want to talk for a moment about what this class of drugs does to Connective Tissues. Yes, the very tissues that desperate (but uninformed) people take these drugs for! Let us talk first about the problems with taking corticosteroids for problems with the Elastic, Collagen-Based Tissues.
Most people who deal with Chronic Pain are well aware of at least some of the dangers associated with taking corticosteroids (cortisone or similar substances). They are also aware that even if corticosteroids help your pain, your doctor will ration the amount that you can receive. There is good reason for this.
Corticosteroids deteriorate (destroy, degenerate, degrade) collagen-based tissue! This is why they are also a known cause things like osteoporosis, Degenerative Arthritis, and other connective tissue problems — the very problems that people are frequently taking the drugs for in the first place! OK, we can all agree that corticosteroids are bad, but what about NSAIDS?
“NSAIDS” stands for Non Steroidal Anti Inflammatory Drugs’s. This is a massive class of drugs, and includes medications such as Celebrex, Naproxen, Ibuprofen, Acetaminophen, Aleve, Aspirin, or any of dozens of other common drugs given for inflammation. Again, it is not that these drugs do not do what they are advertised to do — block inflammation. It is that the side-effects are brutal; and often deadly!
Before Vioxx was pulled from the market, I saw research that touted anti-inflammation medications as being the #13 leading cause of death in the country (see Dr. Gary Null’s DEATH BY MEDICINE). Is that a big deal? Only if you are the one hooked up to a dialysis machine 6 hrs a day, bleeding from your rectum, turning orange from jaundice, or resting quietly six feet underground. If you are one of the people making a living off of the absurd numbers of Americans “living the dream,” its great!
There are several studies that show how injured tissues, when in the presence of anti-inflammatory medications, actually heal up to 1/3 weaker, with 40% less elasticity. NSAIDS are palliative (they relieve symptoms but do not address underlying cause) not therapeutic (actually addressing the root cause of the problem). This is one of modern medicine’s dirty little secrets — not to mention, a huge money maker! NSAIDS will weaken tissue and increase the chances of re-injury. This sets you up for the vicious cycle of Chronic Pain, dysfunction, inflammation, prescriptions of NSAID’s, and more degeneration. Lifelong patients! Talk about job security!
So, let me see if I understand. The very drugs that doctors are giving people to cope with their chronic Deep Somatic Pain; suppress the body’s natural inflammatory response, which is part of the normal healing process. Furthermore, drugs that block inflammatory chemicals are actually causing injury and deterioration of the very tissues that they are supposed to be helping! Am I missing something here? Is it me (after all, I’m just a stupid chiropractor in the RURAL OZARKS OF SOUTHERN MISSOURI), or does this all look like a tospy turvy mish-mash of something piled up in my barnyard?
The truth of the matter is that much of the “practice” of Medicine is not scientific, it is just that — practice. And unfortunately, it has become big business —- very big business. Few doctors work for themselves anymore. They all work for big corporations — here it’s Cox or Mercy. And if you do not believe that “BIG PHARMA” is the puppeteer who is pulling the strings, I have this bridge in Brooklyn that I would just luuuuuuuuuuuuve to sell you!
You should be starting to see why the old model of dealing with injuries to Collagen-Based Connective Tissues like ligaments, fascia, muscles, and tendons (not to mention bones and cartilage), is such a disaster.
We are flushing billions of dollars down the toilet to give people a little bit of symptomatic (palliative) relief, while trading away quality of life, functional recovery, as well as those ‘minimally-important’ organs such as livers, kidneys, stomachs, small intestines, hearts, and the like. Remember the motto of that exercise-loving gal from the late 80’s and early 90′s — the one with the spiky blonde hair? STOP THE INSANITY!
When it comes to understanding and treating Connective Tissue Injuries, we have a medical model that is so outdated, it is literally insanity to continue using it! Stop the insanity —it is clearly time for………
A NEW MODEL OF COLLAGEN REPAIR
Let us look at the new model. Hold on a minute. We should not really be calling this model “new” because none of what you are about to read is new information. As you will soon notice, this is information that has been around for at least a decade — probably more like two or three. This section should really be called, “The Old New Model”. But as we have already talked about, studies say that it takes the latest scientific and medical research almost two decades to get into the text books that doctors learn from.
Realize that although individual Type I Collagen Fibers are all basically the same (see Part I), they can be arranged (woven, cross-linked, etc) into different structures. The different arrangements of collagen fibers are what give it very different properties in different tissues. For instance, in dealing with the Elastic, Collagen-Based Connective Tissues, we see that…..
- Fascia and Ligaments are arranged in “bands” or “sheets”.
- Muscles and Tendons are arranged more like “chords” or “ropes”.
- Aponeurosis are a combination of the two, and are actually considered to be a flattened tendon (which would be like a very thick fascia).
FASCIA
FASCIA is what you get when you arrange collagen fibers into ultra-thin sheets. Think of fascia as similar to a sheet of paper or cellophane. If we were to pick up the sheet of collagen (in this case, fascia) and look at it on edge, it will be very very thin and flat — like a piece of paper. If we picked up the sheet of fascia and looked at it under a microscope, we would see that it is wavy. Fascia has “waves” that give it a great deal of elasticity and stretchiness. This is because individual collagen fibers are wavy. Waves create elasticity, but, what happens if we overstretch or tear this sheet of fascia?
When fascia is overstretched or torn, it tends to “clump” into a wad of twisted and tangled adhesion that we commonly call Scar Tissue. This is easy to understand. Sit down at the table and put both hands out in front of you. Make sure that the palms are flat on the table. Open your fingers up and point the fingers of one hand, toward the fingers on the other hand. Now push the hands together — and pull them apart. Push them back and forth, and notice how the fingers glide effortlessly between each other. This “organized / parallel” structure of the collagen fibers is what gives fascia great elasticity and allows the fibers glide back and forth effortlessly (YOU CAN ACTUALLY WATCH THIS IN REAL-TIME HERE).
Now push the hands together and tangle the fingers from one hand with the fingers from the other. What has happened? Not only do you have little or no flexibility (the fingers are in a tangle), you have a “clump”. This clump is a real problem! Remember how when we turned the fascial membrane on edge, it was flat. When we turn the hands with the clumped fingers on edge, it is no longer flat. The “clump” or “adhesion” (in fascia, I refer to this as a “scar”) creates tangled and twisted tissues that run in all three dimensions. It’s easy to understand why movement in the specific area of the scar will be restricted —- possibly severely.
But remember, not only is this microscopic scarring and adhesion less elastic, it is also extremely pain-sensitive (Part II). The most current scientific literature tells us the scar tissue is not only much less elastic and weaker than normal tissue, but it is up to 1,000 times more pain-sensitive than normal tissue! And the final kick in the teeth is that fasica does not image on MRI — or any other diagnostic test for that matter. Because it does not image, it is not even a diagnostic option for 99% of you struggling with fascial adhesions. Despite this, the medical community continues to perform MRI’s at a record pace (HERE).
Think about it for a moment. Injury (traumatic or repetitive) causes Fascial Scarring & Microscopic Adhesion. Fascial Scarring & Microscopic Adhesion causes extreme restriction and loss of motion. This loss of normal motion causes the nerve system to misfire (loss of proprioception). Loss of proprioception causes Chronic Pain, Degeneration, and it adversely affects the nerve system that controls every function in the body. It is a vicious cycle —– a cycle that is rarely recognized until it is too late — until it becomes a degenerative mess. And even then, your problem will be pawned off on your age
It does not really matter whether you are 35 or 95, your doctor will sit you down, look you in the eye, and solemnly tell you that, “Mrs. Smith; you’re simply not a young as you used to be.” Or you may be told that your problem is “just a little arthritis”. Or better yet, your doctor may tell you that you have DJD. DJD stands for Degenerative Joint Disease, and is really nothing more than a great marketing tool to convince people that they have a “disease”, when the reality is that they have a vicious cycle. The shameful thing is that if your doctor is stuck in the world of the Old Model; aside from some symptomatic care (drugs), your problem will be all but completely ignored!
One more important note before we leave. Although it is not uncommon for people to have “Trigger Points” across their upper back / shoulder area (pain-related small, hyper-irritable knots in muscles), most muscle pain is fascial in origin. And according to research that has been around for decades, many TRIGGER POINTS are directly related to Fascial Adhesions as well. You must also be aware that when people are diagnosed with a “pulled muscle”, about 99% of the time the problem is an overstretched or torn fascia — not an actual tear in the muscle itself.
TENDONS
TENDONS are the Collagen-Based Connective Tissues that anchor muscles to bones. Muscles essentially have two parts. They have a soft central “belly” (the meaty part of the muscle), that is sandwiched between two tough, chord-like tendons on either end. Tendons are very different than fascia. Tendons are not as elastic as fascia (some research says that tendons are non-elastic), and they are “chord-like” as opposed to “sheet-like”. Tendons attach or “anchor” muscles to bones via microscopic velcro-like hooks called “Sharpey’s Fibers”.
For as long as I can remember, problems with tendons have been called “Tendinitis”. But is this really true? Remember the Old Model from part III? The suffix “itis” indicates a primary inflammation. In other words, the problem is said to actually be caused by Inflammation. So, a Tendinitis (sometimes spelled “tendonitis”), by its very name, indicates that the problem in the tendon is being caused by inflammatory chemicals. Doctors will then tell you that the best method for treating Tendinitis with anti-inflammation drugs and Steroid Injections. Although it is true that traumatic tissue injury or repetitive tissue injury can release inflammatory chemicals into the injured area, is inflammation the primary problem, or is it secondary to something else?
Let’s let someone who is far smarter than I am answer that question. World renowned tendon researcher and orthopedic surgeon, Dr. GA Murrell, writing for England’s prestigious Orthopaedic Research Institute; wrote these words that were published as part of an article found in the December 2002 issue of the British Journal of Sports Medicine. The article was called “Understanding Tendinopathies”. Dr Murrell writes that,
“Tendinosis, sometimes called tendinitis, or tendinopathy, is damage to a tendon at a cellular level (the suffix “osis” implies a pathology of chronic degeneration without inflammation). It is thought to be caused by micro-tears in the connective tissue in and around the tendon, leading to an increased number of tendon repair cells. This may lead to reduced tensile strength, thus increasing the chance of repetitive injury or even tendon rupture. Tendinosis is often misdiagnosed as tendinitis due to the limited understanding of tendinopathies by the medical community.”
The more things change, the more they stay the same. According to Murrell’s last sentence, “Tendinosis is often misdiagnosed as tendinitis”. This is no longer true. Patients are being correctly diagnosed. However, diagnosing tendinosis is only being done on paper — for their insurance company.
The reality of the situation is that even though the ICD-9 Code says “Tendinosis” on the HCFA-1500 form that is electronically transmitted to your insurance company, you, the patient, are still being treated in the same manner that you always have — drugs and injections. This is not a good thing, because the suffix “itis” indicates a primary tendon inflammation, as opposed to a primary tendon derangement / degeneration or “osis”.
But like I stated earlier, for the vast majority of doctors, making the diagnosis is nothing more than semantics — choosing language that will get you paid by an insurance company. In other words, they are calling the problem “tendinosis” on paper, and not only using the old language of “tendinitis” with the patient, but they are going about treatment the same way they have for decades —– according to The Old Model. Treatment consists largely of NSAID’s and Cortico-steroids (injections and / or oral).
Think of tendons as “ropes”. These ropes are tough! But after doing the same thing, day after week, after month, after year; the collagen starts to wear. Overworked tendons begin to fray. As you can imagine, this not only causes terrible pain, it causes all sorts of dysfunction as well. And whether the tendinopathy has been diagnosed as “tendinitis” or “tendinosis”, the treatment will surely be the same; and rest assured, it will come straight from The Old Model — NSAIDS and Corticosteroids.
It’s time to stop the insanity! I don’t really care whether you call it Tendinitis, Tendinosis, Banana Boat or Moo Goo Gai Pan; NSAIDS and Corticosteroids are not a good way to treat problems of the Collagen-Based Connective Tissues (whether elastic or non-elastic) period — end of story! There is abundant research (see Part IV for a small taste) that proves that these drugs destroy / eat / deteriorate / ruin Collagen-Based Tissues (whether elastic or weight bearing such as bone)! This is not rocket-science folks!
If anti-inflammation medications are playing any part in your treatment plan for tendinopathy, fascial adhesion, ligamentous scarring, muscle strains, chronic back pain, etc; you seriously need to rethink your treatment protocol! OK. You are convinced. You have done the online research and realize that what I have shown you is true. Hey; it’s not like I came up with any of this all by myself. Like I said, I am just a small-town Chiropractor who has been watching this ongoing battle (New Model -vs- Old Model) for the better part of three decades now. The research is out there for anyone with a computer to find.
For over a decade now, I have been combating chronic Deep Somatic Pain (Part II) by using Scar Tissue Remodeling Therapy to find and treat the adhesions and scarring that are characteristic of injuries of the Elastic, Collagen-Based Connective Tissues. Once I have examined the patient and determined which ranges of motion and which tissues might be affected, Tissue Remodeling allows me to break the adhesions and microscopic scarring so that the tissue can be “remodeled”. Some of the problems that I regularly in my clinic include the list found on our PROBLEMS WE HELP PEOPLE WITH page.

2 Responses
Hello
My question is can Red and near-infrared light therapy help heal these conditions?
You have a wonderful and informative website.
Thank you for all the info you share
Hello Kathy,
Absolutely, although certainly not in each and every case. Honestly the best source for this on my site is my post on Dr Jack Kruse (https://doctorschierling.com/blog/dr-jack-kruse-on-using-light-to-control-ones-weight-and-health) as well as another one that I wrote on the benefits of sunshine beyond vitamin D (https://doctorschierling.com/blog/the-importance-of-sunshine-beyond-vitamin-d). Hope you find this helpful!