
TIGHTNESS, STRAINS, TENDINOSIS AND ADHESIONS
OF THE FASCIA OF THE HIP FLEXOR MUSCLES
A POST IN PICTURES
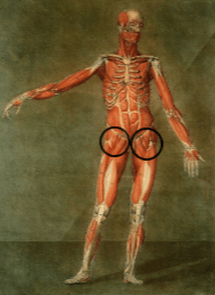
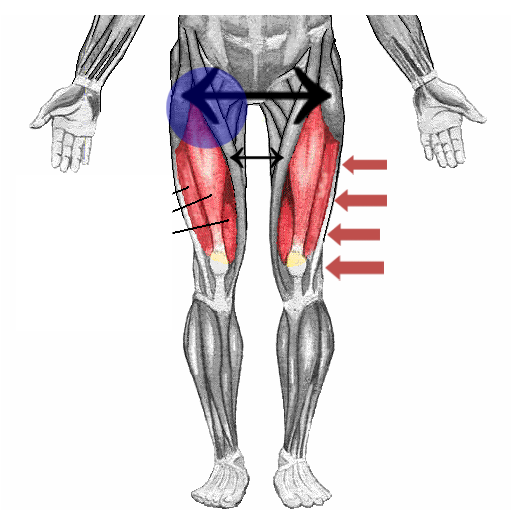
Problems with the Hip Flexor muscles are one of the most commonly undiagnosed / misdiagnosed entities that I see in my clinic. Hip Flexion describes the action of drawing the front of your thigh up towards your abdomen. Although it is not the only place that Hip Flexor muscles cause pain, the most common spot that people experience Hip Flexor pain is in the area marked in the pictures at the top of the page. Today I am going to show you why this is, discuss a few of the potential causes, and talk about ways you can help solve this common problem.
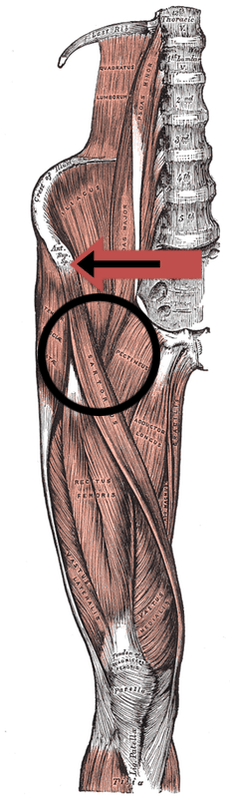
In the picture directly below, you’ll notice some arrows. The large double-sided arrow is pointing to the Tensor Fascia Lata muscle (TFL). The TFL and the Gluteus Maximus (buttock) have a long ‘tendon’ that attaches on just below the knee on the outside part of the leg. This tendon is called the Illiotibial Band or IT BAND, and is labeled with four red arrows (more on it in a moment). The TFL is a very important stabilizer of the hip joint and is often associated with imbalances of the pelvis — particularly short legs. User: Chrizz Many people who go to a Chiropractor or PT are told they have a “short leg”. While having an anatomical short leg (a leg that’s actually short) certainly happens, thankfully it’s not terribly common. What is common is having a functional short leg, or a leg that acts / looks short because the pelvis is in some degree of torque. Either can lead to pain and / or dysfunction in any number of places, including the LOW BACK, the KNEES, and of course, the hips themselves. Be aware that addressing a structural leg length deficiency is going to require some sort of lift. However, using a lift in someone with a functional leg length difference can actually make your problem worse.
The small arrow below the big arrow is pointing to the Sartorius. The Sartorius — the longest muscle in the body — winds its way around from a part of the pelvis known as the ASIS, where it attaches to the inside part of the lower leg, just below the knee. Among the other actions of this muscle, it acts as one of the chief flexors of the hip. Just below and between these muscles, you’ll notice the quadriceps; most particularly the Rectus Femoris, which is one of the most powerful muscles in the body.
Although none of these three muscles (the Sartorius, Rectus Femoris, or TFL) have the exact same attachment point at the hip, they are close enough to each other that I refer to them with patients as the “Common Flexor Tendon” of the lower extremity. And while I certainly find people who have pain in said tendinous attachment (HIP FLEXOR TENDINOSIS), I find that more often than not, Hip Flexor pain is found slightly below that — in the area marked on the picture by the blue circle (many times there will be a small muscular bulge present).
Much of the time people with pain in the blue circle have underlying FASCIAL ADHESIONS. Sometimes the adhesed fasciae will also be found in the large adductor muscles (with the cable-like tendons) that we commonly refer to as the groin. The nice thing about the way I treat is that whether you have Fascial Adhesion or Tendinosis (or more likely, a combination of the two — HERE), we will take care of both at the same time, whichever area(s) it’s found in. Also bear in mind that it is not uncommon to see Fascial Adhesions that cause Hip Flexor pain running all the way down to the knee.
One of the reasons for this is because Hip Flexor and quadriceps tightness is so common. In fact, it’s crazy common here in America, even in people that don’t have Fascial Adhesions, and is mostly due to the fact that as Americans we tend to sit way too much. By keeping our Hip Flexors in a constantly flexed state, we are essentially shortening them, which tends to pull the pelvis forward. How do we solve this?
As I always say, EXTENSION THERAPY is a good starting point for numerous orthopedic / musculoskeletal problems, not simply because of the effects of the stretch itself, but because stretching or exercising in extension fires off critical parts of your brain that are often not under-stimulated (EXERCISE IS THE NUMBER ONE WAY WE STIMULATE OUR BRAINS). As to whether or not you have overly-tight Hip Flexors, a simple THOMAS TEST should answer this (BTW, this test doubles as a stretch). Not surprisingly, I have also noticed a connection between PIRIFORMIS SYNDROME and problems of the Hip Flexor muscles (HERE is an example).
THE SUPERFICIAL AND DEEP
FLEXORS OF THE HIP
 |  |
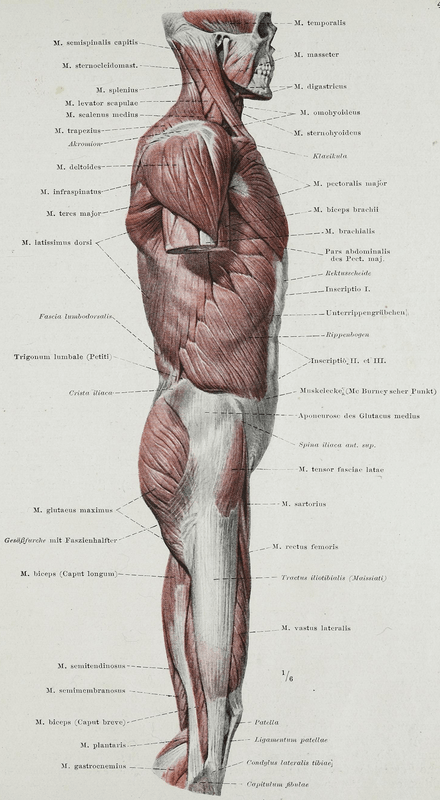
The pics at the top of the page show the muscles and tendons that make up the vast majority of what we usually refer to as a Hip Flexor problem. Any athlete who drives hard off of one leg, while throwing the other leg up and forward in an attempt to gain explosive momentum, runs the risk of developing a Hip Flexor issue (basketball players, football players, soccer players, track athletes, etc, etc, as well as runners or lifters who create similar type situations via overuse). However it is critical to remember that when it comes to Chronic Pain, everything is not always as cut and dried as it may seem. Thus, we can’t leave without discussing both the deep Hip Flexors and the superficial trunk flexors — the later being a muscle group that acts in similar fashion to the former.
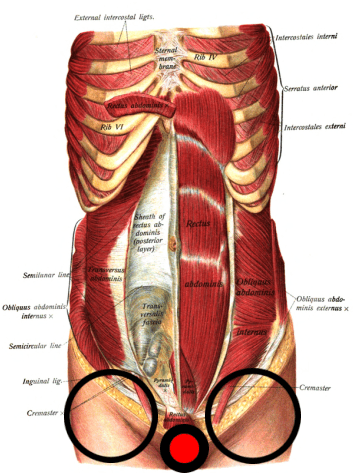
Although the pics for this section were published well over a century ago (Dr. Johannes Sobotta’s 1904 Atlas and Text-book of Human Anatomy), you should notice that the pic on the left shows muscles that are much more superficial (closer to the surface). Pay attention to the several layers of abdominal muscles that run in multiple directions —- vertically (Rectus Abdominus), horizontally (Transverse Abdominus), as well as the Obliques (Internal & External) that run two different ways, exactly opposite each other (if you overlay their fibers, they would form an “X”). Not surprisingly, I have found Abdominal Strains (especially of the lower abdomen) to be associated with Hip Flexor problems (HERE), thanks to similar fascial anchors / attachment points.
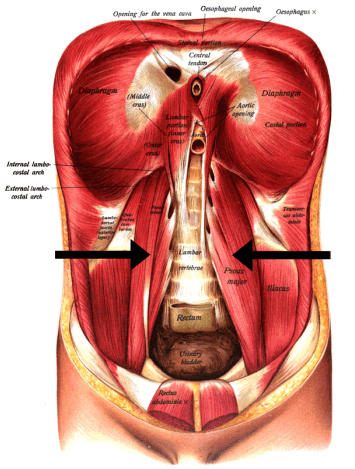
As we peel back the anatomy, remove the organs, and go deeper still, we find the Psoas and Illiacus muscles (often referred to as one muscle; the Illiopsoas) as seen in the picture on the right. This muscle attaches to the lateral portions of the lumbar vertebrae, running downward to anchor itself to the inner part of your pelvis. Unless you are very thin, because your organs overlay this muscle, it is extremely difficult to access therapeutically.
Both of these muscles act as flexors of the trunk (they bring one’s belly and front upper thighs (quads), which is very similar (in many ways almost identical) to flexing the hips. In fact, the extremely powerful psoas muscle is capable of both actions. This is why besides SITUPS AND CRUNCHES being bad for your spine, they tend to work the psoas more than the abs, which can both draw you into a chronically flexed posture (extremely common in the neck as well — HERE). The solution? Forget crunches and / or sitips and do a variety of PLANKS instead. This is particularly true for those of you struggling with CHRONIC LOW BACK PAIN. You will be much better served as far as CORE STRENGTH by focusing on exercises such as yoga, planks, ball exercises, etc, etc, and staying far away from crunches (unless you do them as shown in the previous link).
I also want you to think about the HAMSTRINGS for a moment. Because ‘weak’ hamstrings are almost ubiquitous in the human population — probably because it’s essentially our default state — it’s imperative to your Hip Flexors to keep them (your hamstrings) strong. It’s arguable that the single biggest reason for the explosion of KNEE INJURIES over the past several decades — particularly in youth athletes and most particularly in young female athletes — is directly related to quads overpowering the hamstrings. This is largely because there are so many exercises that work the quads, while you have to be much more intentional about working the hamstrings. However, I do see some patients who develop chronic low back pain simply because their quads are weak.
TENSOR FASCIA LATA PAIN / ILLIOTIBIAL BAND PAIN
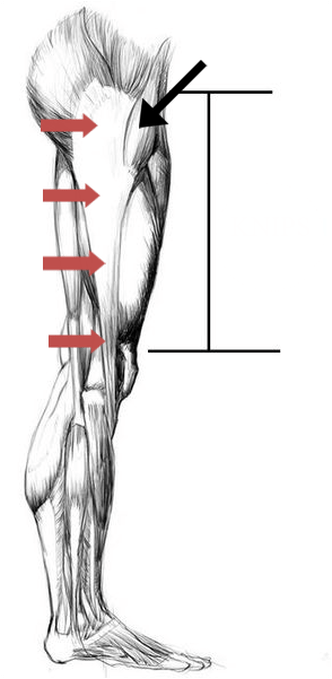 |  |
“The iliotibial band (ITB) or tract is a lateral thickening of the fascia lata in the thigh. Proximally it splits into superficial and deep layers, enclosing tensor fasciae latae and anchoring this muscle to the iliac crest. It also receives most of the tendon of gluteus maximus. The ITB is generally viewed as a band of dense fibrous connective tissue….. “From the March 2006 issue of the Journal of Anatomy (The Functional Anatomy of the Iliotibial Band During Flexion and Extension of the Knee: Implications for Understanding Iliotibial Band Syndrome). The arrow in the pic at the left is pointing to the TFL muscle. The Illiotibial Band or “I.T. Band” is a Hip Flexor with the potential to cause a lot of pain and dysfunction. While this pain can certainly occur anywhere along the length of the ITB, it’s most common painful area would have to be the outer knee (not to be confused with PATELLO-FEMORAL SYNDROME aka Patellar Tracking Syndrome that will be felt at the front of the knee, just below the knee cap). Although the biomechanical causes of Illiotibial Band Syndrome are legion, the most common causes of pain and TIGHTNESS in this area are crappy or incorrect footwear for your specific foot type, EXERCISING ON HARD SURFACES, weak or improperly firing hip / buttock muscles (particularly Gluteus Medius), and just plain overuse. What do we know about overuse as it pertains to connective tissues — particularly tendons?
Although we know that tendons do actually inflame (HERE — for years the medical research community said they did not), the most common form of tendinopathy is ‘degeneration’ or ‘derangement’. The medical word to describe this phenomenon in tendons is “TENDINOSIS“. Because doctors usually treat the problem as an “itis” —- most often attacking it with THE BIG FIVE instead of things like TISSUE REMODELING or DRY NEEDLING that are geared toward addressing the underlying “osis” or derangement (often associated with TRIGGER POINTS as well) — it’s no wonder that their treatments so often fail.
As a side note; although I am a fan of foam rollers (cheap, easy, and DIY), make sure to test your Glute Medius first to see if it’s weak (HERE’S HOW). In similar fashion to the Thomas Test above, you can use this same action to strengthen the muscle. Bear in mind that of all the muscles and tissues associated with hip flexion, the IT Band is where you’ll by far find the most variance as far as what the experts say you should be doing to solve your problem.
PICTURES OF MOST COMMON
AREAS FOR HIP FLEXOR PAIN
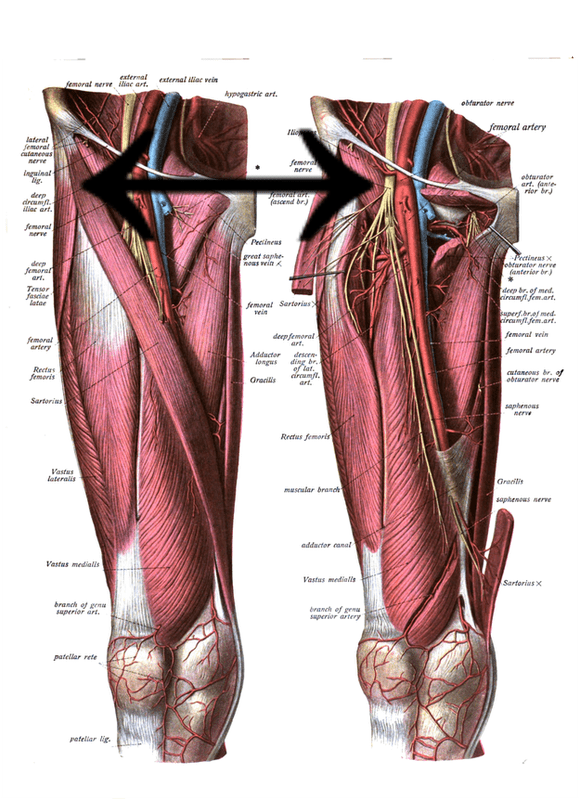
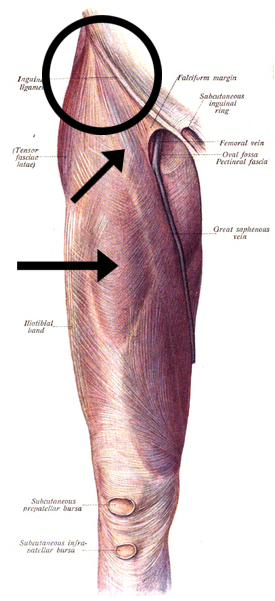
BELOW LEFT: The red and black arrow shows the ASIS; a heavy duty bony attachment point on the very front of the pelvis. Although the Rectus Femoris muscle (middle quadriceps) anchors itself just below the other two muscles (Sartourius and Tensor Fascia Lata), I refer to this area, including the circle, as the Common Flexor Tendon. BELOW MIDDLE: This double-arrow shows the area I often refer to as the Common Flexor Tendon of the lower extremity. BELOW RIGHT: This is an awesome picture of the surface anatomy of the region we are discussing today, that actually shows the FASCIA covering the muscles of the thigh. Notice that both muscle and Fascia has a grain to it — sort of like wood does. I have A POST that deals with this grain as it pertains to Fascia, which is known as “Langer’s Lines of Cleavage”.
 |  |  |
If you have been dealing with CHRONIC PAIN of any of the areas that make up the Hip Flexor, there are some things you might try before coming to see me. For one, STRETCHING has a huge upside. Just be aware that if stretching makes you worse, you almost surely have FIBROSIS / SCAR TISSUE / ADHESED FASCIA. Also, if the problem is relatively minor, you might be able to solve it with a FOAM ROLLER. Realize that there are dozens of YouTube videos showing an array of different stretches and exercises for the Hip Flexor group.
Secondly, do whatever it takes to eliminate inflammation in your life. INFLAMMATION comes in numerous forms and is the root of virtually all problems in your body. Fail to address underlying Inflammation and you are much more likely to fail as far as solving your pain is concerned. And thirdly, if you are a runner or hardcore lifter, you may have to make some changes in how you train. In fact you might actually have to take a little bit of time off for things to heal — particularly true with the IT Band. For those who can’t take any time off, there are other options. HERE’S ONE EXAMPLE of a female pole vaulter who had pain for over two years prior to coming to see me (one visit), and HERE’S ANOTHER EXAMPLE of a one-visit “cure” in a man who had his Hip Flexor problem for over a decade and a half.
If you like, feel free to at least look at the generic template I created for helping people get out of pain, solve their chronic health issues, and get their lives back. The really nice thing is that THE PROTOCOLS ARE ESSENTIALLY THE SAME simply because most disease process and chronic pain process are essentially the same (HERE). And if you thought this post was valuable, why not share the wealth by liking, sharing, or following on FACEBOOK. It’s not only the most effective way to reach those you love and care about most, it’s the easiest as well.

{kind=link}