
TORN OR ADHESED FASCIA
WHAT IN THE WORLD DOES IT LOOK LIKE?
Invisible. At some point in their life, everyone has secretly (or maybe not so secretly) desired to be invisible. There are a couple of all-too-common situations within the medical field, however, where being invisible is a bad thing — potentially a very bad thing. While our national epidemic of “INVISIBLE” biomedical research is an international disgrace, today we are going to focus on MUPS — medicaly unexplained physical symptoms. Although there are many reasons a person might end up with MUPS, arguably the most common, at least musculo-skeletally speaking, has to do with FASCIA.
Because fascia does not image with standard technology (HERE), struggling patients are frequently treated as though their problem / pain doesn’t exist — as if IT’S ALL IN THEIR HEAD. It’s also common to be treated as a drug seeker, especially in the environment surrounding our ever-present OPIOID EPIDEMIC. The result is patients who live in despair, often times being told their pain is the result of DEPRESSION, when the opposite is far more likely to be true. What’s exciting is that for many of you reading today’s post, there is hope. There may actually be a way to start breaking out of the prison of HELPLESSNESS / HOPELESSNESS and STRESS your pain has confined you to.
Today I want to show you a picture of a FASCIAL ADHESION that’s caused several years of CHRONIC PAIN (9 on a scale of 10) in a woman who had tried everything under the sun in an attempt to not only treat, but simply figure out what was wrong with her. The problem started several years ago as the result of OVER-VIGOROUS STRETCHING, which caused a “popping” sound, intense pain, and later, hardness in her lower abdomen (yes, soft tissues will often pop when they TEAR OR BREAK).
Although over the course of her ordeal she was given a myriad of ever-changing diagnosis (including CUTANEOUS NERVE ENTRAPMENT(S)), she was eventually told she had INTRA-ABDOMINAL ADHESIONS, ultimately ending up having them surgically removed (she’d had several past abdominal surgeries, including more than one vertical C-section, which were, excepting an appendicitis surgery, decades old), which helped a great deal with the feeling of hardness and internal abdominal pain. Unfortunately, the severe pain above her right lilac crest (the bone you put your hands on when you put your hands on your hips) was still there, only worse.
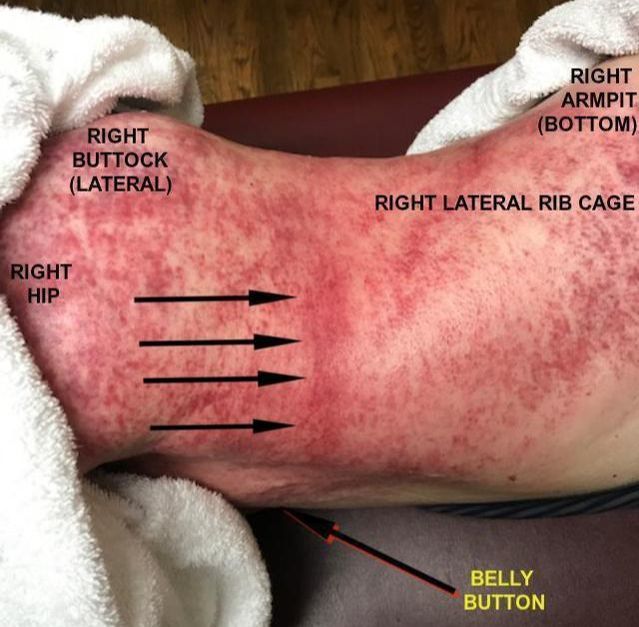
I tested and found areas of restriction, and in her case decided to work my way in towards the epicenter of her pain instead of working my way out (part of my reasoning was that she had extremely tight HIP FLEXORS and a great deal of pain in her upper buttock / hip / lower back — I did not find much adhesion in her THORACOLUMBAR FASCIA). Since sitting was what reproduced the most pain (sitting was never pain-free for her), I would work on an area, then have her walk around a bit. I would then have her sit for a little while to see if her pain had changed (I call this BULLSEYING).
Before I ever got to the epicenter (the four arrows), her pain upon sitting had reduced substantially. As I worked my way in, I found two quarter-sized areas of ADHESED FASCIA which were obviously TETHERING HER substantially. Upon breaking them, her pain diminished even further. right next to these I found THE TEAR ITSELF (click for a pic of a different patient), which ran ran almost from her navel to her spine (you can visually see some of it in the picture above).
After working on this area, the patient could not reproduce pain. I gave her the proper stretching protocol and she and her husband started their journey home, with her riding in the back of a van so that she could stretch and pull the HAIRBALL-LIKE tissues apart before the broken adhesion could re-adhese. For the record, her husband was in the room with us for the entirety, the towel on her hind end was tucked into her underwear, and even though it’s cut off in the pic, she was wearing a bra that had been pushed up, with a towel stuffed underneath.
I am not completely sure whether or not these results will hold up for her but SHE WILL KNOW AFTER THIS ONE TREATMENT whether or not that’s the case. Not surprisingly, however, when a patient leaves my clinic unable to reproduce the pain that has been turning their life upside down, it’s a hopeful sign. Will she have to return for more treatment? I have no idea. Regardless, we found her problem, allowed her to visualize it (important because IF IT BLEEDS, WE CAN KILL IT), and began the process of breaking down the SCAR TISSUE and FIBROSIS. If she does have to return, her next visit will be much shorter and easier (I spent an enjoyable hour and a half with she and her husband, learning the history of the area they hail from). And no; not everyone I treat has this kind of scar tissue, or for that matter, any significant scar tissue at all.
The scheduling slots for the OUT OF STATE & INTERNATIONAL PATIENTS I treat are, for the most part, reserved for Tuesday and Thursday mornings so that I can spend whatever time may be needed to address whatever we happen to find. While I cannot guarantee a “cure,” browse through a few of the hundreds of PATIENT TESTIMONIALS on our site, some in the form of letters or emails, and others in the form of videos that we mainly do in-house (although on occasion someone sends me something they shot on their phone). Quite a few of these testimonials are from long-distance patients, but the majority are from the folks I treat right here locally (Springfield, Mountain Home, Rolla, and Poplar Bluff are all only an hour and a half away).
Also be aware that my average patient is not going to leave the office looking like this. Many patients simply need the right CHIROPRACTIC ADJUSTMENT to resolve their problem(s). However, if you are not holding your adjustments like you feel you should be (HERE), it’s a common sign that there may be invisible scar tissue and adhesion present. For those who may be wondering, HERE is what a typical “First Visit” will look like for a local patient. It costs nothing to talk to me to see if I think I can help.
Because you must never forget how intimately inflammation is related to scar tissue (HERE), and that there are things you can be doing to address your level of systemic inflammation (HERE) —- or that adhesed fascia is believed by a growing number of experts to be THE ROOT OF ALL PHYSICAL AILMENT — it might behoove some of you to click the links in this paragraph. Finally, if you are one of the folks enjoying the mountains of free, relevant, and cutting-edge health-related information found on my site, be sure and spread the wealth. One of the best and easiest ways to reach those you love and care about most is by liking, sharing, or following on FACEBOOK.
