
KNEE TESTIMONIALS
KNEE TESTIMONIALS TIM OSBORNE BARB KING KAREN HELTON MICHAEL SMITH MICHAELA SCHIERLING My knees were hurting bad every time that I played soccer. It was

KNEE TESTIMONIALS TIM OSBORNE BARB KING KAREN HELTON MICHAEL SMITH MICHAELA SCHIERLING My knees were hurting bad every time that I played soccer. It was
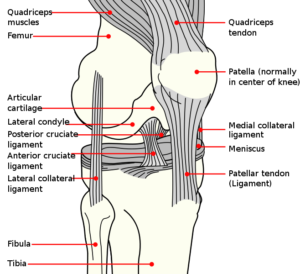
KNEE TENDINOSIS https://staticxx.facebook.com/connect/xd_arbiter.php?version=44#channel=f2ee6a0e9c&origin=https%3A%2F%2Fwww.doctorschierling.com When we talk about Knee Tendinosis, there are two distinct kinds. To understand this, you need to understand a little bit

Leg Stretches THIGH / QUADRICEP / HAMSTRING / KNEE STRETCHES / OSGOOD SCHLATTER SYNDROME STRETCHESHIP FLEXOR & ABDOMINAL STRETCHES These are the stretches for the

KNEE TENDINITIS / KNEE TENDONITIS “Tendinosis, sometimes called tendinitis, or tendinopathy, is damage to a tendon at a cellular level (the suffix “osis” implies a
CHRONIC KNEE PAIN?SURGERY NOT USUALLY THE BEST ANSWER “The benefits of knee repair procedures in older adults for painful
THE GROWING PROBLEM OF KNEE PAIN “Recent Center for Disease Control and Prevention (CDC) and National Center for Health Statistics (NCHS) data suggest substantial rates

DOES KNEE SURGERY CAUSE KNEE ARTHRITIS?SEEMS SO “The meniscus is needed to distribute the body weight across the knee. Without the meniscus the body weight

“I HAVE BECOME MY KNEE” Becky Stern I‘ll never forget the first time I heard a patient make a statement like this; “I have become

“….hell, into the fire that shall never be quenched—where their worm dieth not….” -The words of Jesus Christ from Mark 9:43-44 Let me start by
Centralized Pain or Not? Why Understanding Chronic Pain and Central Sensitization is Critical in Your Personal Battle with Pain “For society, the costs are staggering:

Does Pain Cause Problems in Fascia, or Do Problems in Fascia Cause Pain? “You might attribute a painful neck or a backache to tired muscles

Addressing Densified or Thickened Fascia to Address Chronic Pain Although I have been discussing THICKENED FASCIA on my site for at least 15 years (oftentimes
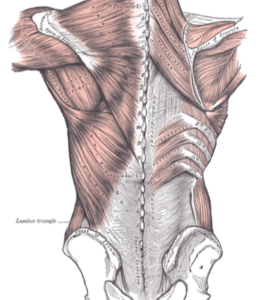
The THORACOLUMBAR FASCIA is arguably the single hottest area of study as far as low back pain is concerned. With LBP being almost ubiquitous in

Although Cassie’s case was extremely common as far as what was wrong with her (FASCIAL ADHESIONS caused by SEVERE TRAUMA had caused unbearable neck pain,
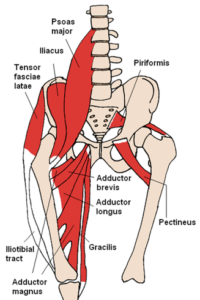
HIP FLEXOR TENDINOSIS & GROIN TENDINOSIS A FEW OF THE HIP FLEXOR TENDONSSOMETIMES THE GROIN MUSCLES / TENDONS ARE CONSIDERED HIP FLEXORS As you might

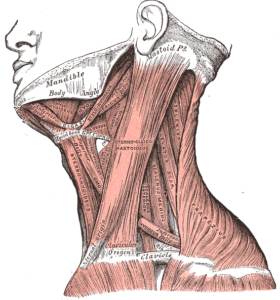
DEGENERATIVE ARTHRITIS & ITS RELATIONSHIP TO LOSS OF PROPRIOCEPTION Osteoarthritis Maybe your NECK HAS BECOME TERRIBLY STIFF? Maybe your neck has not moved like
Understanding the Problems We Help Having managed a wide variety of patients and their various Chronic Pain Syndromes here in Mountain View since early 1992,

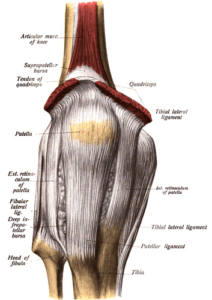
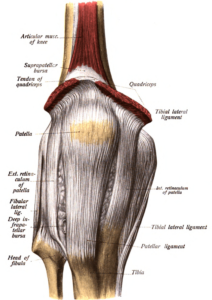
WHAT IS CHIROPRACTIC AND WHAT MAKES SCHIERLING CHIROPRACTIC, LLC DIFFERENT? BASED ON THE OLDEST MEDICAL TEXTBOOK STILL WIDELY IN USE TODAY: GRAY’S ANATOMY Dr. Schierling

QUADRICEPS TENDINITIS, PATELLAR TENDINITISQUADRICEPS TENDONITIS, PATELLAR TENDONITIS “Tendinosis, sometimes called tendinitis, or tendinopathy, is damage to a tendon at a cellular level (the suffix “osis”
PIRIFORMIS SYNDROME & LOW BACK STRETCHES PIRIFORMIS SYNDROME is a potentially devastating form of deep buttock pain that is often associated with SCIATICA (leg pain).